Obligate intracellular (cannot make ATP - uses host cell ATP)
Infection of epithelial cells lead to granulomatous response
Not seen on gram stain - peptidoglycan layer lacks muramic acid
Elementary body is the infectious form of the bacteria (has attachment proteins) - gets into the host cells anc converts into reticulate body which replicates and then converts back to elementary body to infect more cells
Apresentação clínica
Trachoma - serotypes A, B, Ba and C
Developing endemic countries
Follicular conjunctivitis leading to scarring and inturned eyelashes leading to corneal scarring and blindness
Not recommended if used doxycycline in uncomplicated patients
Recommended if pregnant or persistent symptoms. Best timing 4 weeks.
Cannot be cultured on inert media - intracellular (use tissue cultures or embyonated eggs)
Self collected swabs similar sensitivity, more convenient
Gram stain
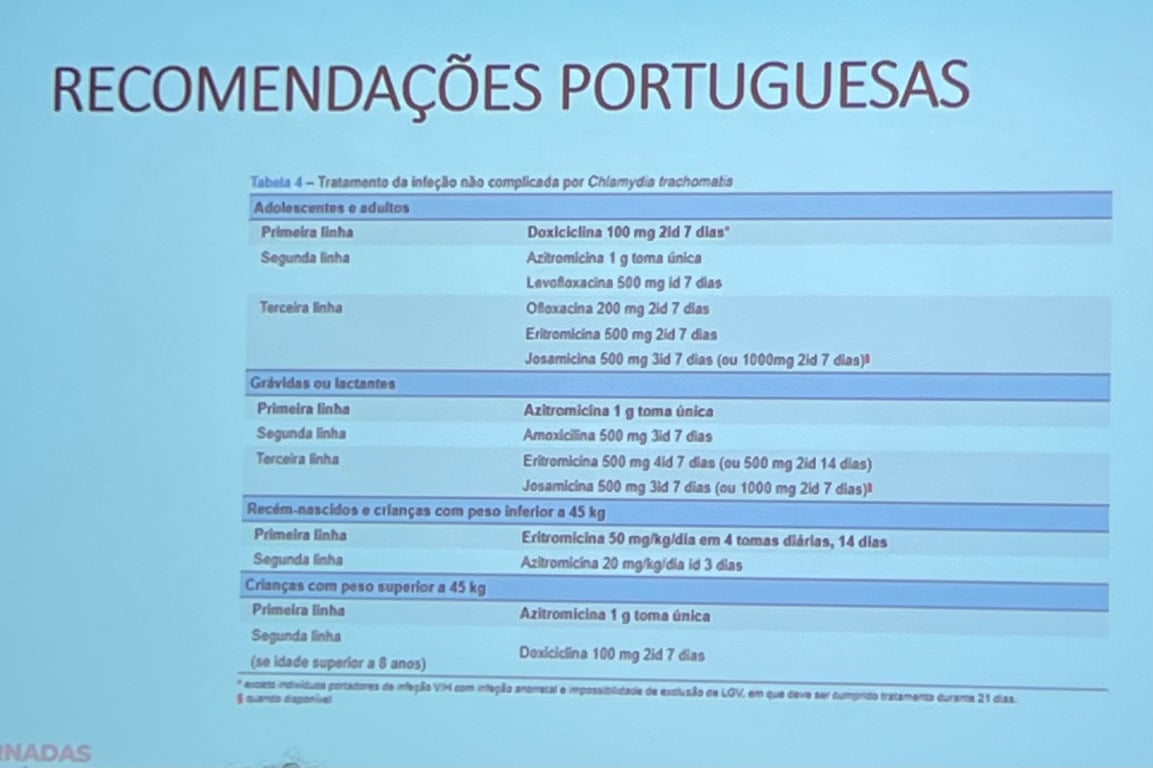
Tratamento
No evidence of any stable homotypic genetic and phenotypic anti microbial resistance in C. Trachomatis
Treatment failures: poor compliance, reinfection, TOC too early
Partner treatment: expedited partner therapy without testing? STIs other than chlamydia will be missed.
Adolescentes e adultos
1st line
Doxycycline 100mg 2id 7 dias
2nd line
Azithromycin 1g stat - causes problems in resistance to other organisms like gonorrhoea and mycoplasma
Levofloxacin 500mg id 7 dias
3rd line
Ofloxacina 200mg 2id 7 dias
Erythomycin 500mg 2id 7 dias
Josamicina 500mg 3id 7 dias (ou 1000mg 2id 7 dias)
In pregnancy ou lactemtes
1st line: azithromycin 1g toma única
2nd line: amoxicillin 500mg 3id 7 dias
3rd line
Eritromicina 500mg 4id 7 dias (ou 500mg 2id 14 dias)
Josamicina 500mg 3id 7 dias (ou 1000mg 2id 7 dias)
Recém nascidos e crianças com peso inferior a 45kg
1ª linha: eritromicina 50mg/kg/dia em 4 tomas diárias, 14 dias
2ª linha: azitromicina 20mg/kg/dia id 3 dias
Crianças com peso superior a 45kg
Azitromicina 1g toma única
Doxicicina 100mg 2id 7 dias
Prevention
Screening
Controversial
No evidence that screening for chlamydia and gonorrhoea in asymptomatic patients lowers the prevalence of these infections in MSM.
Argument in favor of not testing: we also don’t test for meningococcal carriage in oropharix
DoxyPEP
Local pentamidine prophylaxis against Chlamydia trachomatis
Vaccination
No vaccine currently available
1960-70 - studies with live attenuated vaccine showed incomplete protection and increased inflammation, which could lead to infertility. Later efforts were much more cautious
Vary candidates are being studied (mRNA vaccine, Trachoma “prime-pull” vaccine strategy)
 Made with Bullet
Made with Bullet