No cell wall → all betalactams are intrinsically resistant
Few available anti microbial classes: macrolides, quinolones, stropogramins, tetracyclines
Antimicrobian resistance
Global concern
Collateral effect of chlamydia management
Mediated by mutations
A2058G and A2059G (E coli numbering) > 90%
Diagnostics
PCR based tests. May be combined with resistance to macro lide resistance.
Most are Low quality. Currently, the best are 3 FDA/CE-IVD approved high-throughput M. Genilalium NAATs: Hologic Altima, Roche Cobas, Abbott Alinity
Roche Liat (newer in 2025, better, will be available, but no macrolide resistance results)
Detection of macrolide resistance mutations should be performed in all positive samples to guide treatment (several guidelines) to shorten duration of infectious news and limit use of moxifloxacin
Numerous approaches with laboratory developed and commercially available assays (SpeeDx, Pathofinder, SeeGene) to look for macrolide sensitivity
If a test is not available, ask the patient if they got a macrolide antibiotic in the last year
Diagnostics manufacturers uncritically include commensalism as urea plasmas and M. Hominids in STI pannels
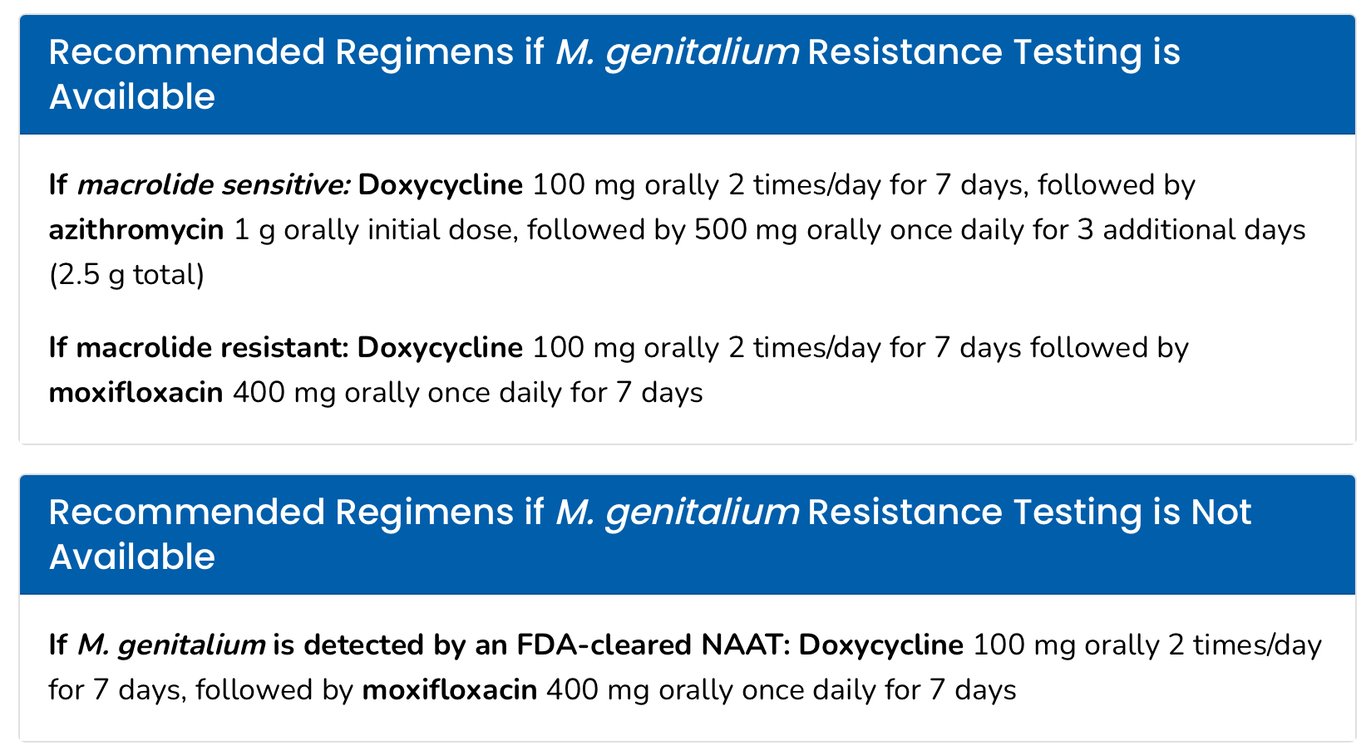
Tratamento
The only well evaluated antibiotic is moxifloxacin 10 days
Quinolone resistance is raising (specially in China)
Testing for quinolone resistance are not predictive of treatment failures (MIC variable, detection of mutation doesn’t mean tretmanet failure), so is not recommended
Pristinamucin 1g 4-10 days
Safe in pregnancy
Consider combining with doxycycline (non pregnant)
Minocycline 100mg x2 2-14 days, 70% cure
Combine with metronidazole 400mg x2
Sitafloxacin 100mg x2 7 days (70% cure)
Pleuromutilins
Lefamulin (50% cure), company went bankrupt
Gyrase/topoisomerase inhibitors
Nitroimidazoles
Metronidazole and tinidazole (slightly more effective than metronidazole)
Some effect in combination effect
Other Tetracyclines
Omacycline and eracycline appeared (?)
Evaracycline only available in and expensive
Amphenicols
Chloramphenicol
Thiamphenicol is a safer alternative
Has been used for STIs
Much better PK/PD properties than CHL
M3P (minocucline, metronidazole, methenamine, pristinamycin) 14-28 days
Aggressive cocktail but patients tolerate quite well
 Made with Bullet
Made with Bullet