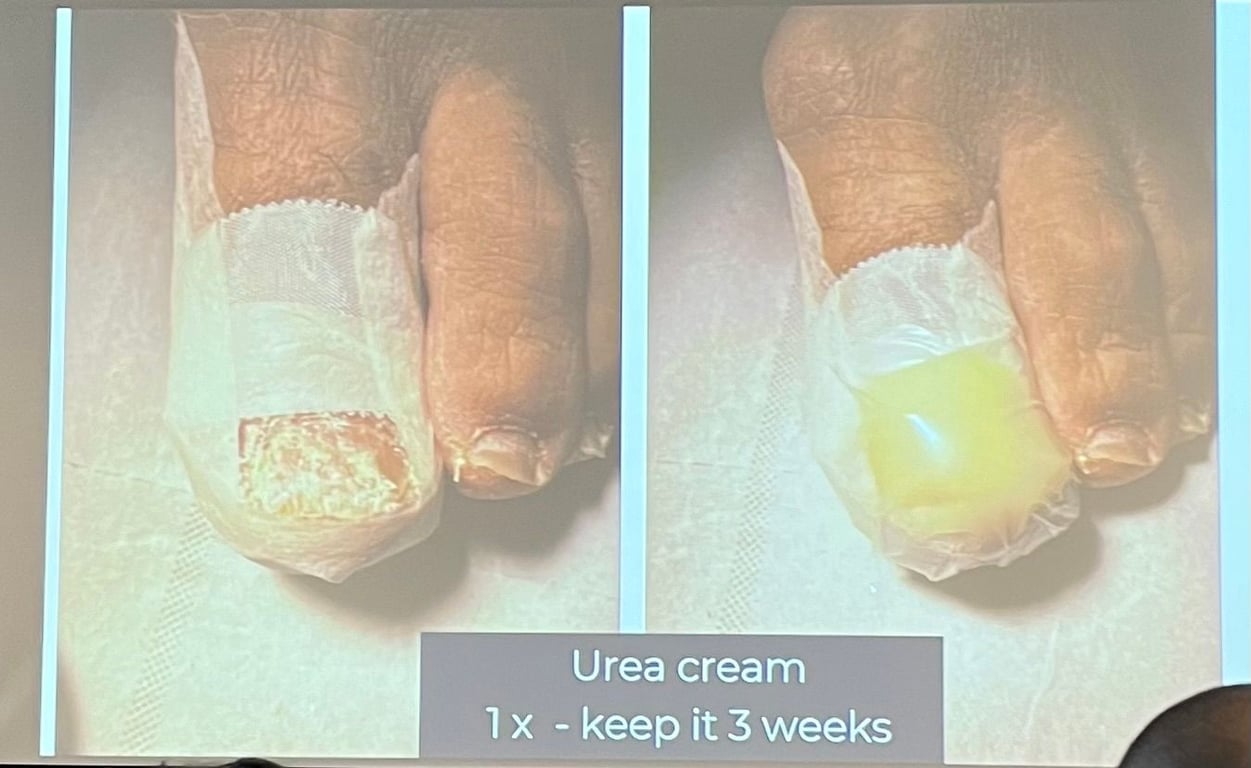
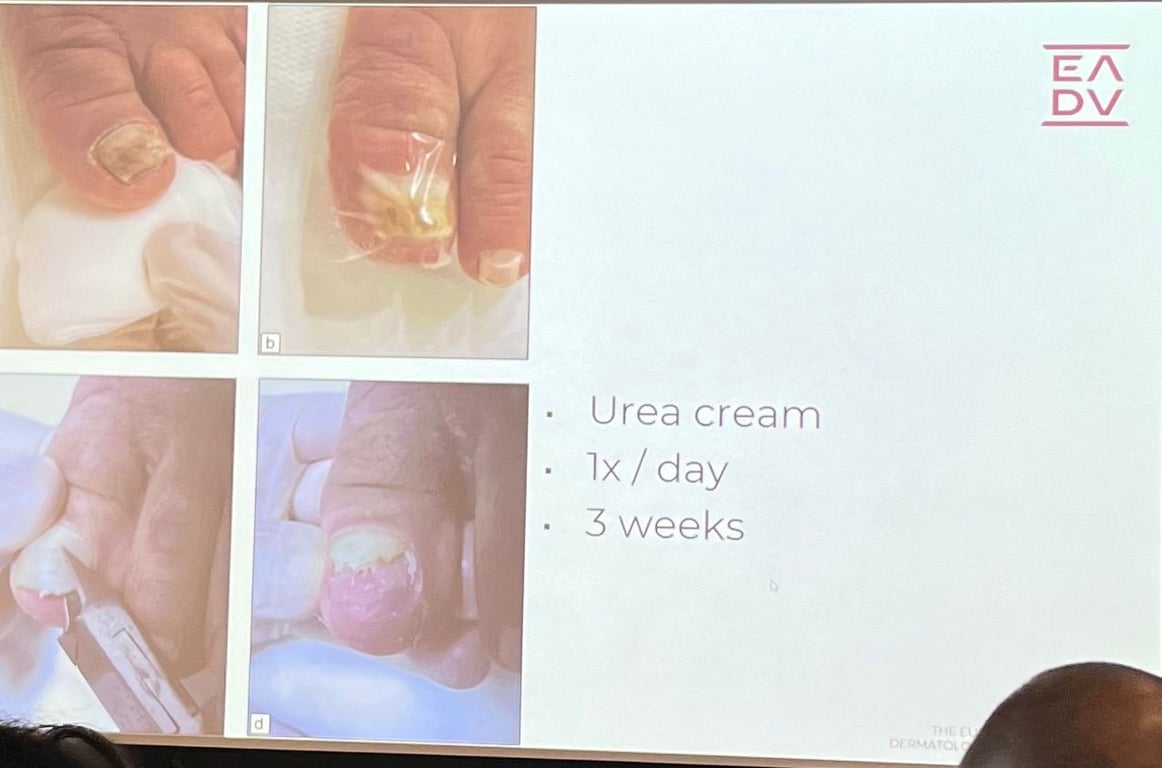
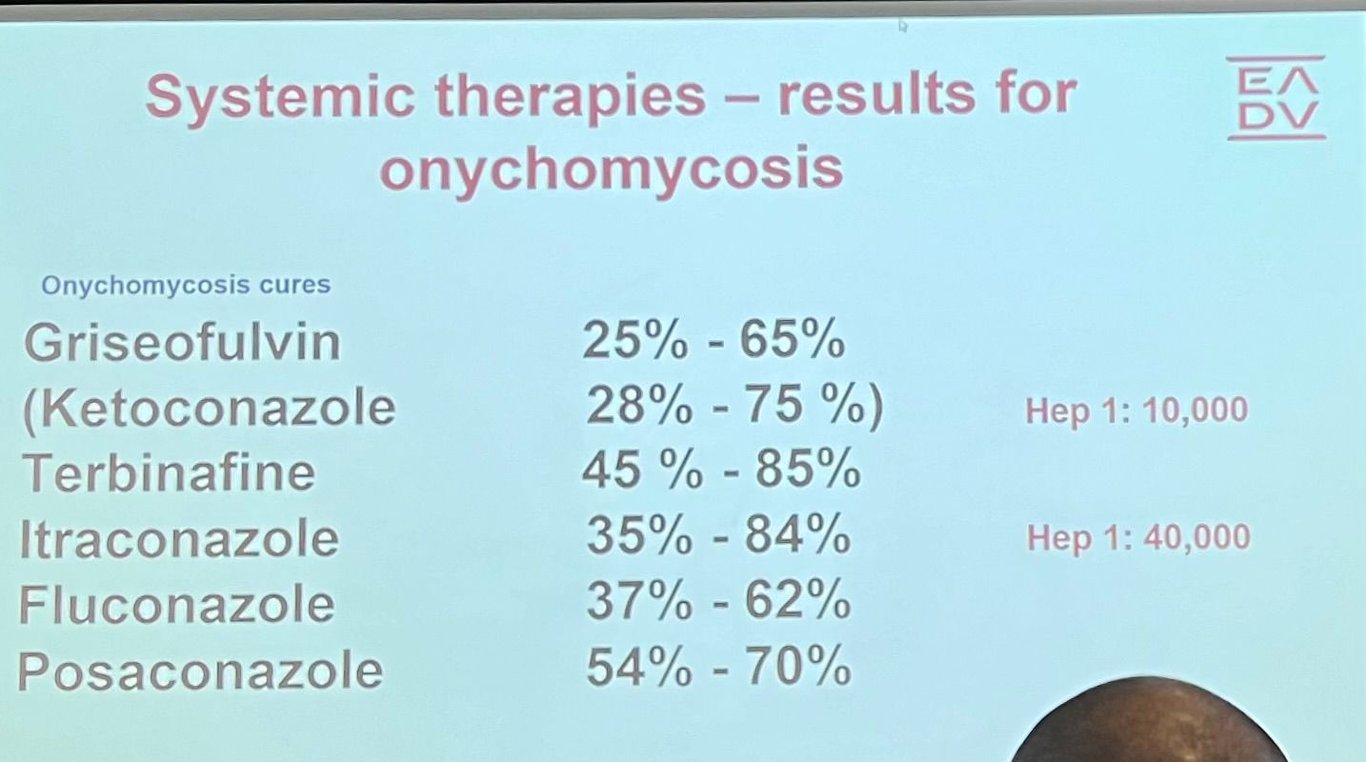
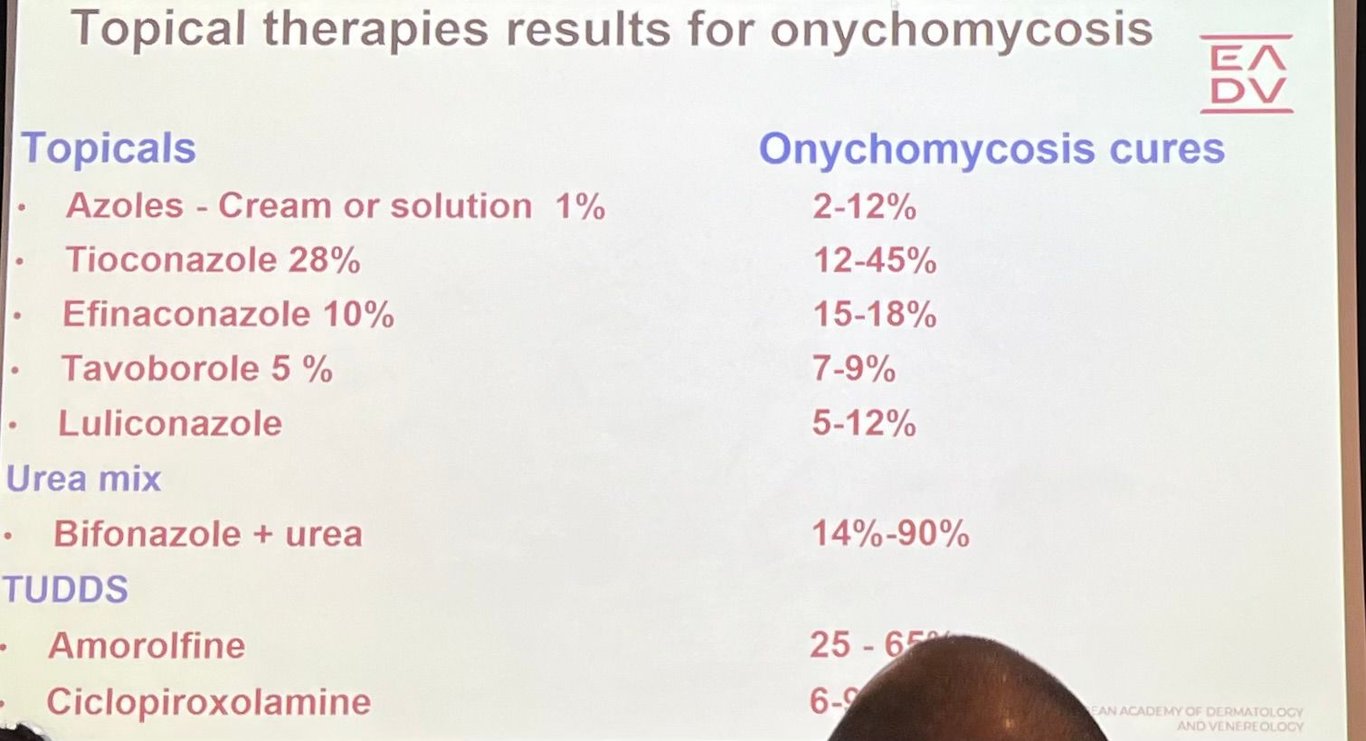
Onychomycosis Epidemiologia 50% (only) of all nail disorders seen in clinical practice Worldwide prevalence of 5,5% Toenails 7x > fingers If an onychomycosis is suspected, 3% of patients will be subject to a nail sampling (Guibal F et al J Mycol Med 2009; 19:185-90) → useless, long and expensive treatment and side effects Etiologia T. rubrum is most common Microsporum canis - gato ou cão Trichophyton verrucosum - gado Apresentação clínica: Estrias longitudinais perpendiculares ao bordo anterior da unha, pode ser amarelado. Na psoríase é mais em mancha. Espessamento e debris subungueal Pode ter pigmento, alguns fungos produzem pigmento Apresentações mais resistentes ao tratamento Large onycholysis Lateral form - o bordo lateral da unha vai mais profundo e é mais difícil de tratar Longitudinal strike - dermatophytoma, if you cut it it goes indent the skin of the nail plate Non-dermatophytic molds Subtipos 2014 new classification - Baran R, Hay RJ. New classification for onychomycoses. J Mycol Med. 2014 Dec;24(4):247-60 Subungueal distolateral Hyperkeratosis Onycholysis Melanonychia Paronychia Superficial branca Classic (dorsal patches) Atypical Emergence below the PNF Proximal leukonychia Deep invasion Mixed Proximal subungueal Procurar imunodeficiência: primária, HIV, medicação Paronychia Pseudo-candidosic Candidosic Moulds Dermatophytes Without paronychia Punctate leukonychia Transversal leukonychia Longitudinal proximo-distal leukonychia Endonyx ++ fingers after scratching tinea capitis toes with friction from shoes Primary or secondary total distrophy Systemic form Deep lymphatic extension Secondary systemic dissemination Candida DDx Only 50% of abnormal nails are fungal!! Test before treating Lichen planus Trauma Psoriasis Eczema Contact dermatitis Norwegian scabies Pseudomonas infection? Hematoma Sinais de alarme para suspeitar de outras causas Distrofia ungueal com culturas negativas Padrão atípico Falência de tratamento Dermoscopy Spikes Subungueal hyperkeratosis “Jagged edge with spikes” and striae - study by professor with beautiful hair Maria Bianca Piraccini Leukonychia Distal pulverization or ruin appearance Pigmentation (could be due to the fungus or inflammation) Aurora borealis pattern (antonella tosti) Diagnóstico: nail sampling is mandatory High quality sampling is keystone Performed by the physician himself Send to a trustworthy mycology lab Basic prerequisite Topical antifungals stop 3-6 m Systemic antifungals - stop 3-6m Avoid contamination (bacteria, moulds, yeasts) - alcohol 70-100% wash before Remove as much as possible of infected keratin up to the clinically healthy area (”mycelium front”) If Superficial - scraping (blade, curette) If Distal lateral subungueal: wide clipping, subungueal curettage If Proximal subungueal - punch Document Number of nails affected Toenail, fingernail Clinical signs (drawing) Suspected diagnosis Sampling Samples kept dry in an envelope Send by post too the lab Survival time 2-4 weeks Exames de diagnóstico: Cultura do debris subungueal Raspar com bisturi ou cureta o debris subungueal ou cortar a ponta da unha com alicate de unhas Apanhar o raspado com uma lâmina e usar outra lâmina tipo sandwich Embrulhar em papel e colocar etiqueta a fechar Enviar para laboratório com requisição de cultura Sensibility 70% Raspado para exame direto com KOH Biopsy or nail clipping with PAS stain Sensibility 94% Pathogen location - if superficial in an old patient consider only topical therapy DDx: psoriasis, mychomatricoma, scabies, trauma Min retangulo 3*4mm Não precisa de meio, pode ir seco PCR Tratamento Não é OBRIGATÓRIO tratar Erradicate maximum fungal load Mechanical techniques Chemical techniques: urea 40-50% Surgical Tratamento oral Cura clínica só em 50% dos doentes Terbinafina 250mg id 3 meses se unhas nos pés Dose adapted in children, liver or renal dysfunction Not during pregnancy and breastfeeding (Cat B) Alternativa: 1 mês seguido e depois 1 semana por mês durante 5 mês Alternativa: pulso de 250mg id 7 dias repetido a cada 2-3 meses até cura Alternativa: pulso de 500mg id 7 dias por mês durante um total de 3 meses EADV Mycology Copenhaga Terbinafine pulse therapy 2 cycles 250mg/day (4 weeks on, 4 weeks off) 500mg/day, 7 days/month during 4 consecutive months 500mg/day, 7 days every 3 months, totaling 4 treatments Terbinafine Booster Therapy Additional 250mg/day during 4 weeks, 6-9 months after original full treatment course for patients with a bad prognosis Itraconazol No serviço: Normal é 200mg por dia pode ir a 400 se infeção mais grave Curso EUA: 200mg BID durante 1 semana por mês durante 2-4 meses Estágio espanha: 400mg id 1 semana por mês durante 3 meses AN a meio do tratamento Fluconazol 150mg por semana durante 6 a 12 semanas Duração: 1,5 mês se nas unhas das mãos 3 meses se nas dos pés Children: terbi>itra>fluco Tratamento tópico (receita médica) Verniz na unha, creme no leito ungueal Duração LONGA, caros, eficácia limitada (12-18% dos casos) Eficácia do tratamento depende da rapidez de crescimento da unha Ciclopirox id 6 meses nas mãos, 9-12 meses nos pés Niogermos, mycoster (é comparticipado - 5€) mas existem outros (diário) - 6.6mL ou 3.3mL fazer a noite para deixar 6h a atuar sem contacto com água Dexulac Amorolfina (1x/semana mas piores resultados) Ureia tópica 40-50%, deixar durante 3 semanas com opsite ou 1x/dia 3 semanas. Já há kits comerciais ex onyster Candida onychomychosis Fluconazole 150-450mg once weekly x 6 months Itraconazole 200mg daily x 6 w (hands) or 12 w (feet) or 400mg x days/months x 2-3 months (hands) or 3-4 months (feet) Medidas gerais Cortar as unhas rente Ventilated shous Limit heat and humidity Hygienic feet Meticulous drying Weating washable or disposable shoes in the bathroom Shoes disingection Terbinafine cream or antiseptic soap weekend therapy Avoid stagnant water Plastic shower mat
 Made with Bullet
Made with Bullet