Contact dermatitis is a skin inflammatory reaction caused by direct contact with a harmful environmental agent
Eczema implies inflammation in french terminology.
Historically: Contact Eczema = Allergic contact dermatitis, but Irritant should be just dermatitis as is non-allegergic.
However, new insights in pathophysiology show irritant also recruits immune system. New classification of allergic diseases proposed defining both entities as delayed hypersensitivity reactions (DHSR)
Historically: Contact Eczema = Allergic contact dermatitis, but Irritant should be just dermatitis as is non-allegergic.
However, new insights in pathophysiology show irritant also recruits immune system. New classification of allergic diseases proposed defining both entities as delayed hypersensitivity reactions (DHSR)
Epidemiologia
- Difficult to establish
- Lifetime prevalence of hand eczema = 9%
- 1 year period prevalence of 7.3%
- Point prevalence of 3.2%
- Point prevalence of contact allergy = 15%
- Most common contact allergens: nickel (8.6%) & fragrance mix (1.8%)
Classificação
Dermatite de contacto irritativo (80%)
- Fisiopatologia: efeito citotóxico direto, imunidade inata
- non-specific release of junk from damaged cells triggers TNF-alfa, but many other immune pathways emerging
- No sensitization required
- Infrequent exposure to strong irritants or frequent exposure to milder irritants
- Often occurs in atopic dermatitis due to impaired barrier and lower irritant threshold
- Commons exposures: frequent hand washing, hand sanitizers, harsh soaps (e.g. antibacterial), heavily fragrant skin care products
- Frio e pouca humidade diminuem o conteúdo de água no estrato córneo e aumentam a permeabilidade a irritantes. Contudo oclusão aumenta a humidade da pele e aumenta a permeabilidade de irritantes solúveis em água
Dermatite de contacto alérgica | Eczema de Contacto (20%)
- Fisiopatologia: reação de hipersensibilidade retardada tipo IV, imunidade adquirida
- Allergen crosses skin-barrier
- The allergen can be an hapten → a small molecule that requires interaction with a biological macromolecule (eg. a protein) to induce allergy
- Haptens may have characteristics that allow easy penetration of epidermis (lipophilicity and low molecular weight)
- Some molecules only become reactive during skin metablism → prohaptens
- binds to Langerhans cells (APC of skin), which present the antigen in HLA at the membrane, migrate to regional lymph nodes (eg. axilla)
- The exposure of the antigen results in activation, recruitment and expansion of T cell clone that are specific that have memory to this substance, which circulate in the blood.
- Exposure to antigen in another part of the body or skin will recruit memory T lymphocyte which has epidermotropism and will cause eczema there
- Overlap with some pathways involved in atopic dermatitis
- IL9 and IL17 have been implicated
- In the old days, used to think allergic contact dermatitis was Th1 and atopic dermatitis was Th2 but now known that both are implicated in both diseases
- Food/seasonal allergies are immediate reactions (minutes to a couple of hr), with mast cell, IgE, histamine mediated and risk of anaphylaxis
- Allergic contact dermatitis is delayed reaction (days, sometimes even weeks), lymphocyte mediated, not IgE or histamine mediated (except contact urticaria) and no risk of anaphylaxis (except contact urticaria)
- Previous sensitization required: sensitization may occur after infrequent exposure to strong allergens or frequent exposure to milder allergens
- Once sensitization occurs, even minimal exposures can be provocative
- Delayed reactions involving lymphocyte recruitment/expansion
Photo allergy
Photo toxicity
Diseases caused by contact allergens
- Eczema
- Erosions
- Ulcerations
- Urticaria
- Erythema multiforme
- Purpura
- Lichenoid eruptions
- Exanthemas
- Erythroderma
- Allergic contact granuloma
- Lymphocytoma
- Sarcoidal reactions
- Toxic epidermal necrolysis
- Pigmented contact dermatitis
- Contact leukoderma
- Nodular lesions
- Photosensitive reactions
- Generalized symptoms
- Contact urticaria may become anaphylaxis
Anamnese
- Existe alguma predisposição - ex. Dermatite Atópica?
- Existe alguma exposição possível - sazonal, variações diurnas, dias de trabalho vs fim de semana?
- Qual a severidade?
- Perguntar relação com atividade profissional e férias
Apresentação clínica
- Limites bem definidos localizado no local de contacto com o alergénio
- Placa eritematosa vesicular ou descamativa (epiderme)
- Prurítica
- Nas pregas as lesões são foliculares porque o alergéneo penetra mais facilmente nos folículos e poupa a prega que é mais húmida e mais propícia para os fungos
- Se aguda: vesículas, edema, exsudação
- Se crónica: liquenificação, descamação
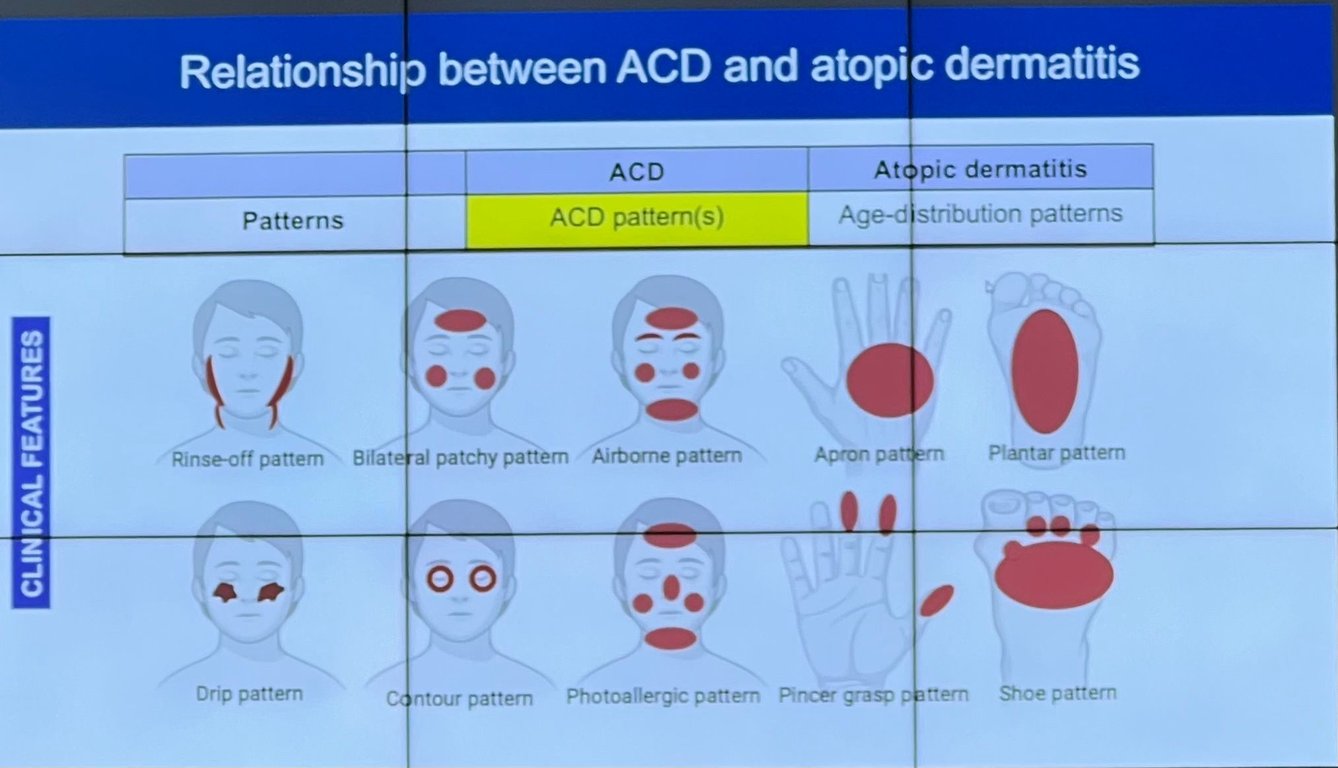
- Padrão clínico: contacto direto, airborne, administração sistémica, generalização
- Contacto directo
- Airborne
- Achados simétricos.
- Distribuição: áreas expostas da pele
- Na face (pálpebras, conjuntiva, sulco retroauricular), pescoço, peito, mãos, pulsos, antebraços, flexuras (axilas, antecubitais, poplíteas), nas mulheres às vezes também as pernas
- Etiologia: ex: cromatos do cimento aerosolizados, resinas epoxy na indústria
- Eczema de Contacto por via Sistémica
- Via: Oral, intravenoso, intranasal
- Oral
- Dieta rica em níquel: oysters, herring, tea, mayonnaise, vegetables cooked in stainless steel cookware
- AINEs ex etoricoxib → pode-se dar celecoxib
- Intravenoso: injeção de imunoglobulinas
- Intranasal
- Manifestações clínicas
- Baboon syndrome → rash in gluteal and inguinal region
- Mimetizar eczema atópico
- Eczema disidrótico
Causas
- Organizados em grupos
- Alergénios e agentes específicos
- É o mais frequente no mundo (poison Ivy é o mais frequente nos EUA)
- iPads, iPhones, game controllers where rubber band comes off,
- Benefits of nickel: relatively cheap, prevents corrosion, prevents tarnishing, low magnetic permeability (prevents microwaves), temperature resistance, increased strength of metal
- Ear piercing is the strongest risk factor for developing nickel allergy
- Jewelry alternatives: platinum, 24 karat gold (pure), 985 silver, better stainless steel alloys (have nickel but retain it better)
- Foods considered high in nickel: chocolate, cocoa powder, mussels, licorice, hazel nuts, almonds, peanuts, walnuts, soy beans, oatmeal, wheat
- Low-nickel diets to treat dermatitis with positive patch test to nickel → controversial (Bolognia)
- Dimethylglyoxime test: test to see if products are releasing nickel
- Most commonly used preservatives
- Used since 1930s
- They are active against bacteria, yeast, fungi, and algae
- Widely used in: personal, household, industrial products, medications (oral, topical, injectable), foods
- Generally safe, well tolerated with low irritancy and allergenicity, but concern about estrogenic properties, but never really confirmed, but replaced for the following preservatives
- Preservantes - Active against bacteria, yeast, fungi and algae
- First introduced in 1980
- Widely used in personal, household and industrial products: cosmetics, especially shampoos, moist toilet paper and baby wipes (anogenital reaction), sunscreens, hair gels, household cleaning products, anti-bacterial washes, topical medications, makeup removals
- Atualmente proibido em cosméticos de pessoas mas pode estar nos cosméticos de animais
- Active against bacteria and fungi
- First introduced in 1980s in europe and 1990s in North America
- Widely used in personal, household, and industrial products: soaps, shampoos, detergents, creams, sunscreen, ultrasound gel, wet wipes and moist toilet paper
- Active against bacteria, fungi, and arachnids
- They are widely used in wood preservative, but has been progressively used in paints, metalworking fluids, household products and cosmetics
- Relatively uncommon preservative, but positive patch test reactions are frequently encountered
- A lot of irritancy and should be interpreted with caution
- Not found in the TRUE test
- Prof Margarida: muitos falsos positivos
- Topical medicaments, cosmetics or intralesional or intravenous anesthetics
- Metassulfito é um pó branco que se coloca nos vinhos, procurar na etiqueta se contem sulfitos
- Lanolin (wool fat, wool grease, wool wax, wool alcohol) is a natural product obtained from the sebaceous glands of sheep
- Emollient properties
- Used in many topical medicaments and cosmetics
- More common in patients with chronic dermatitis (atopic dermatitis, stasis dermatitis, cheilitis). Keep in mind when recommending products in these patients (eg aquaphor)
- Uroshiol - poison ivy, poison oak, sumac - most common in USA, not routinely tested
- Figueira e ruda - pensar em fitofotodermatose, a apresentação é muito parecida
- Acrilatos por exemplo no cimento das cirurgias a coluna, dentistas (próteses dentárias), unhas de gel, extensões de cabelo
- Nas pomadas xeriproct e cremes para as hemorroidas que tem lidocaine para anestesiar. Ver região perianal. Geralmente são mais as amidas que dão do que os ésteres
- Ultraproct é uma pomada com lidocaína e pode ser usada em doentes com alergia só a cinchocaína
- Carvone é um produto de oxidação de limoneno.
- Pode estar nas pastas de dentes.
- Pode causar Granulomatose orofacial
- Pó de talco é inerte, não dá dermatites de contacto
- Tiurans
- Carbamatos
- Mercaptobenzotiazole
- Tioureias
- Nos testes epicutâneos
- Pode fazer “edge effect” - mais concentrado no centro, vê-se mais na periferia
- Ler ao 7º dia
Níquel
Parabens
Methylisothiazolinona / Methylchloroisothiazolinone (MCI/MI)
Euxyl K400 (methyldibromoglutaronitrile/phenoxyethanol)
Iodopropynyl butylcarbamato
Sodium metabisulfite
Lanolin
Cainas
Limoneno
Borrachas
Corticosteroides
Diagnóstico
- Testes de alergia - generalidades
- A dose de prednisolona não deve exceder os 20mg
- Don’t do screening → too many allergens, doubtful relevance
- Não escolher fazer o teste em áreas que estão inflamadas ou estiveram inflamadas recentemente
- Contraindications: pregnancy, severe general illness, current allergic disease, infection of suspected organ, ingestion of reaction-inhibiting medications, risk of difficult-to-manage reaction, lack of emergency supplies
- Skin tests
- Rub, scratch, prick and intracutaneous tests
- The lest risky skin test
- Used when a marked hypersensitivity is expected or native materials are tested
- The test material is placed on the inner aspect of the forearm and then rubbed 10 times in a roughly 3cm circle
- Typical test materials are animal hairs, plants, foods, natural latex, medications, cosmetics and skin care products
- A negative control - cotton pad clipped in normal saline (0.9% NaCl solution) is rubbed in the same way
- Reading after 20 minutes
- Both erythema and wheal are considered positive
- The inner aspect of forearm is scratched for 1cm without drawing blood
- The test substance is applied to this minor defect
- It can be a medication or a food, often fround with a mortar and pestle and then mixed with normal saline
- Controls: normal saline and histamine
- Reading after 20 minutes, 6 and 24 hours
- Both erythema and wheals are considered positive
- The most widely used skin test
- Drops of standard allergen solutions are placed onto the inner aspect of the forearm
- The the skin is pricked through the drops with a lancet to a depth of 1mm, without drawing blood
- Controls: normal saline and histamine
- Reading after 20 minutes, 6 and 24 hours
- Both erythema and wheal are considered positive
- Variants: testing on the back and pricking directly through test substances such as foods
- 0.02-0.05mL of sterile, more diluted allergen solutions are injected intracutaneously on the forearm
- This approach may increase the sensitivity of the test
- Allows quantification of the reaction by further dilutions (in the case of bee and wasp toxins)
- And may be used to evaluate delayed hypersensitivity reactions
- Typically the prick test soltions are further diluted 1:10-1:100
- Controls: normal saline and histamine
- Reading after 20 minutes, 6 hours and 2-4 days
- For testing delayed hypersentivity tuberculin or candidal antigens are most frequently employed
- Both erythema and wheal are considered positive
- Mechanical urticaria can lead to false positive
- suspected contact dermatitis
- Other types of chronic dermatitis (eczema) not improving with treatment
- Skin and mucous membrane eruptions (including delayed-type drug eruptions) in which delayed-type hypersensitivity is suspected
- Severe or generalized active dermatitis
- Systemic immunosuppressive treatment
- Dermatitis on the upper back
- Test sites recently treated with topical corticosteroids (7 days prior)
- Recent ultraviolet (UV) exposure of the test area
- Patch testing during pregnancy or lactation is not known to be harmful, but most dermatologist postpone testing as precaution
- Upper back is preferred
- Also: outer suface of the upper arms or thighs
- Weak positive (+): erythema, infiltration, papules
- Strong positive (++): also discrete vesicles
- Extreme positive (+++): also bullous or ulcerative reaction
- Doubtful reaction: faint macular, no infiltration, homogenous erythema
- Irritant reaction: discrete patchy erythema with no infiltration
- Pigmented reaction: considered na overlap with lichenoid contact eczema
- Timing
- Eritema pigmentado fixo lê-se no dia seguinte
- Fototestes também se lêem as 24h
- toxidermias le-se por vezes ao 7o dia
- corticoides le-se ao 7º dia
- Pode fazer “edge effect” - mais concentrado no centro, vê-se mais na periferia
- se alguma leitura duvidosa ao 3o dia, ou algum fármaco importante e tudo negativo
- restantes lê se ao 3o dia
- Mixed in vaseline or water
- Conserved at 4ºC, protected from light
- Atopy patch test
- In patients with atopic dermatitis, aeroallergens such as house dust mites, pollens or animal hairs may cause not only hives but also dermatitis when applied under patch test conditions
- Indications for atopy patch test
- Suspicion of aeroallergens or food allergy when predictive specific IgE levels and skin prick tests are negative
- Severe persistent atopic dermatitis with unknown trigger factors
- Multiple IgE sensitisations of unkown clinical relevance
- Native foods, SPT (skin prick test) solutions on filter paper and purified allergens in petrolatum have been used for APT
- The European Task Force on Atopic Dermatitis has developed standard protocol
- Larger 12mm chambers
- Occlusion time, readings and evaluations - as for standard patch test
- Photopatch test
- Prof Margarida
- UV-A: 1, 2, 5 J (habitualmente até 15 ninguém reage)
- UV-B: 30, 60, 100, 150 mJ
- A duplicate set of allegens is prepared and applied on two corresponding areas of the back
- After 1 or 2 days of occlusion, one set of tests is irradiated with 5J/cm2 of UVA while the other is completely shielded from light and kept protected until further reading
- The 1-day occlusion/reading is usually used in photobiology clinics, whereas contact dermatitis clinics use 2 days of occlusion before irradiation
- UVB can additionally be used to irradiate one set of allergens: it is recommended first to determine reactivity to UVB light (phototests performed on the day of application of the patches), and the UVB dose for irradiation of the test site should be only 75% of the patient’s minimal erythema dose
- Readings and evaluation - as for the standard patch test
- Repeated Open Application Test (ROAT) - “poor man’s patch test”
- Standardized exposure test mimicking a use situation
- Aim to induce allergic contact dermatitis in the test area
- With this method it is possible to clarify the clinical importance of selected patch test reactions
- Test solutions, either commercial products or special test substances are applied twice daily for 2-4 weeks on the flexural (volar) aspect of the forearm near the antecubital fossa
- The size of the test area is usually 3x3 to 5x5cm and the amount of test substance should be sufficient to cover the test area
- The applications continue until a reaction develops or until the end of the selected exposure period
- It may be advisable in selected case to include a control substance on the contralateral arm and the ROAT may also be performed in a blinded fashion
- Semi-open/open test
- Mainly for testing patient-supplied products with suspected irritant properties (shampoos, detergents, paints, varnishes, cooling fluids, pharmaceuticals and some cosmetics)
- A small amount (~15microL) of the product is applied with a cotton swab on area (1cm2) of the skin (on the flexural (volar) aspect of the forearm)
- Allowed to dry completely
- Checked for signs of contact urticaria after 20-30 min
- Then for semi-open test covered with permeable tape and for open test the place is left uncovered
- Then readings are performed at D2, D3 or D4
- Patch testing of patients’ own materials
- Leave-on cosmetic preparations, protective creams and topical medicaments can usually be tested “as is”
- Rinse-off cosmetic products such as liquid soap, shampoos and shower gels can be tested at concentrations of 1-10% in aqua
- If possible - test individual components of the patients’ own products separately
- The test concentration of any individual ingredient in a product to be tested should not exceed the recommended test concentration for this substance
- Check the pH and adjust it with buffers before testing
- Multitest
- The forearm is the preferred site. Other sites can be employed
- An induration of more than 2mm is positive
- The individual values are summed, giving a score (total number of mm of positive reactions)
- Norm in central Europe - 5mm for women and 10mm for men
- Less suggests an immunodeficiency
- Excessive reactions suggest repeated exposure to an allegern
- Subcutaneous provocation testing can be employed when routine skin testing and in vitro studies have failed to clarify a history that stongly indicates a potential allergy
- Only substances that are designed for subcutaneous injections should be used
- Contraindications: pregnancy, infancy, current allergic disease, infection of suspected organ, ingestion of reaction inhibiting medications, severe general illnesses, risk of difficult to manage reaction, lack of emergency supplies
- Do with a functioning intravenous line
- Emergency services should be immedely available
- Typical injection site is the extensor surface of the upper arm opposite the side where the intravenous line is placed
- First a placebo injection with normal saline to assess the emotional and stress related response
- Starts with 1/10 of the normal dosage, and then doubles the dose every 20 minutes until the comulative normal dose is reached
- Both the subjective symptoms and objective signs induced by the test are recorded: local erythema, swelling, elevated blood pressure and increased pulse rate
- Pitfals:
- False-positive reactions: opiates, histamine-rich foods, mechanical urticaria
- False-negative reactions: anaphylactic shock, corticosteroids, immunosuppressants, antihistamines, psychotropic agents
- Physical urticaria tests
- Dermographism
- Pressure
- Cold
- Heat
- Sweat
Rub test
Scratch test
Prick test
Intracutaneous test
Testes epicutâneos / patch testing
Should be considered in patients with:
Postponing if:
Bad | Medium | Good |
Prednisone >10mg/d (20mg in Bolognia) Intramuscular triamcinolon/betametasone (avoid 4 weeks) Topical corticosteroids or calcineurin inhibitors (avoid 1 week) Azathiprine, cyclosporine, mycophenolate mofetil, systemic tacrolimus | Methotrexate Prednisone <10mg/d TNF inhibitors Ustekinumab Antihistamines | Dupilumab, tralokinumab, lebrikizumab JAKi Crisaborole |
Location
Reading:
Substances
Quando há eczema atópico/das mãos e há um alergénio suspeito, faz se prick test, as vezes são moléculas maiores que o patch test não consegue detetar
Subcutaneous provocation tests
- In vitro tests
- Indications:
- Skin or provocation tests are not possible (pregnancy, infancy, medications, active disease, high risk from in vivo testing)
- In vivo tests are unclear
- Exact definition of the allergen is sought
- Types of tests
- Nitrocellulose strip
- Radioallergosorbent test (RAST)
- Enzymelinked immunosorbent assay (ELISA)
- only useful for orientation purposes
- also seen in parasitic infections, pulmonary aspergillosis, congenital immunodeficiencies, immunosuppression, graft vs host reaction, indirectly in HIV/AIDS and even severe burns
- Released by activated eosinophils by degranulation
- Has cytotoxic and neurotoxic effects, reflects the degree of eosinophil activation, decreases with effective antiallergic therapy
- Normal value is less than 105ng/mL
- Elevated levels of ECP can be identified in the blood and other bodily fluids in some clinical settings
- Immediate hypersensitivity reactions
- Parasitic infections
- Non allergic rhinitis
- Eosinophilic syndrome (NARES)
- Nasal polyposis ECP
- Is released from mast cells during a type I reaction, reflects the degree of mast cell activity
- It is more stable than histamine and easier to identify
- The physiological function of tryptase is not well-understood, but it appears to play a role - as does kallikrein - in making bradykinin available
- Also known as the histamine releasing test
- Basophils are isolated from the patient’s blood and then mixed in a test tube with the suspected allergen for 30 minutes
- The histamine content is then measured
- To provide positive and negative controls, basophils from a patient known to be allergic to the substance and from a normal, nonallergic individual must be tested in parallel
- Basophils from patients with allergic disease are often sensitive and degranulate in a nonspecific fashion
- Is similar to BDT but the release of leukotrienes (D4, C4 and E4) from leukocytes is measured
- Because these products are synthesized de novo following exposure to the specific allergen, the test is less likely to be influenced by nonspecific stimulation
- CAST is more exact than the specific IgE measurement and is only employed in type I reactions
- is useful when searching for antibodies such as anti-pigeon serum antibody (pigeon breeder’s lung) or anti-Aspergillus antibody (pulmonary aspergillosis)
- The test serum is placed in a well in the center of an agar plate and the antigen in varying concentrations is placed in the surrounding wells
- The antigens and antibodies of the sera diffuse toward one another through the gel
- If specific antibodies are present in a given serum, antigen-antibody complexes form, leaving a precipitation line
- Is used to identify the antigen spectrum
- Used for the identification and standardization of allergen extracts that are used for prick tests, provocation tests and hyposensitization
- Is used to identify the antigen pattern
IgE directed against specific allergens
Total IgE
Eosinophilic cationic protein
Tryptase
Basophil degranulation test (BDT)
Cellular allergen stimulation test (CAST)
Immunodiffusion (Ouchterlony method)
Crossed Immunoelectrophoresis
Crossed radioimmunoelectrophoresis
- Provocation tests
- Types:
- Oral, Skin (patch, prick tests) are the ones used by dermatologists the most
- Conjunctival, nasal, bronchopulmonary
- Modified provocation tests are needed:
- When inhalation provocation tests are carried out either at the work place or under standardized conditions
- When oral provocation test is combined with increased physical activity
Histologia
- Pode ser necessária para DDx com Micose Fungoide
- Lymphomatoid Contact Dermatitis → the clinical and histopathologica aspects suggest a similarity to mycosis fungoides
- Padrão de dermatite espongiótica, pode ter eosinófilos
Tratamento
- Abordagem aguda no SU
- Excluir celulite
- Corticoide tópico +/- oral (com IBP)
- Saurat: prednisolone 15mg/day 3 days, then 10mg/day 3 days,, then 5mg/day 3 days
- Medrol 24mg 5 dias e para (Duarte Flor em doente com eczema grave nos braços)
- Diprosone
- Consulta de seguimento
- Considerar consulta de testes
- Tratamento em consulta
- Identificar e evitar o trigger
- Contact allergen Management Program (CAMP) allows members to input known allergens and the database assembles a list of products free of the allergens entered
- Medidas específicas por área afetada
- Corticoide em SOS
- Tacrolimus tópico
- Metotrexato (off-label)
- Ciclosporina (off-label)
- Azatioprina (off-label)
- Dupilumab (off-label)
- Em investigação
- Gusacitinib
- Delgocitinib (tópico)
- Eczema de contacto irritativo
- Biafine
 Made with Bullet
Made with Bullet