Neuroendocrine, lymphotropic, radiosensitive, immunogenic, aggressive malignant tumor
Linhagem
- Not truly derived from normal Merkel cells
- Meckel cells are mechanoreceptos found in the basal layer of epidermis (face, palms and soles) and hair follicles
- Merkel Cell Carcinoma originate from dermal stem cells, epidermal progenitors, or fibroblasts that undergo transformation into a neuroendocrine phenotype
- “Merkel Cell Carcinoma derives from a pluripotent stem cell that has acquired the ability to differentiate into a malignant neuroendocrine phenotype” (Saurat)
AEIOU rule
- Asymptomatic
- Expanding rapidly
- Immunosupression
- Older than 65 years old
- UV exposed sites
Etiologia
- Virus: Merkel cell polyomavirus (MCPyV) (80%)
- UV-induced mutations (20%)
- Imunosupressão aumenta o risco 24x
- LLC aumenta 30-50x o risco
- Advanced age
Apresentação clínica
- Rapidly growing purple/red nodule or plaque in sun exposure areas
Histology
- small cell neuroendocrine appearence
- small blue cels
- Imunohistoquímica
- Marcação neuroendócrina (ex. CD56, sinaptofisina e cromogranina A)
- Marcadores específicos do Merkel (outros neuroendócrinos não)
- CK20 (with characteristic perinuclear staining)
- Marcadores negativos no Merkel, positivos noutros neuroendócrinos
- TTF-1 → small cell lung cancer
- CK7 → small cell lung cancer
- Pode marcar poliomavírus
- pode ter diferenciação divergente, isto é, ter uma parte do tumor diferencia-se noutro tumor - CEC, triquilemocarcinoma, etc. O Merkel que tem diferenciação divergente não marca poliomavírus, ao contrário do Merkel puro
- Poupa a derme papilar (Grenz Zone)
Estadiamento
- AJCC8 TNM staging
Prognosis
- 5year OS 45% in stage cI to 13,5% in stage IV
High risk features
- Size ≥2cm
- Chronic immunosuppression
- Head/neck primary site
- Positive lymph node
- Lymphovascular invasion
Pre opterative staging procedure
- US of regional nodes
- Whole body imaging: TC CTAP or PET
- No brain imaging needed
Management of primary
- Primary tumor
- Surgical therapy with 1cm safety margin followed by RT on the tumor bed
- Margem >1 vs. <1cm não afeta a sobrevivência se associada a RT adjuvante
- Adjuvant RT should be preformed within 8 weeks
- Tumor is highly sensitive to radiation. Dose ~50Gy in 2Gy per fraction
- Sentinel lymph node biopsy should be done
- If SLNB negative → no RT on lymph node
- If positive SLNB (microscopic nodal disease): adjuvant RT alone (50-55 Gy) or eventualy combined with CLND
- If macroscopic nodal disease: therapeutic CLND should be performed
- Adjuvant treatment should be discussed in multidisciplinary team (nivolumab)
Management of locally advanced or metastatic disease:
- immunocompetent patients with locally advanced or metastatic MCC shall receive anti PD1 based immunotherpy as first line treatment
- Pembrolizumab (anti-PD-1)
- Nivolumab (anti-PD-1)
- Avelumab (anti-PD-L1)
- Case “Lokale Tumorkontroolle eines metastasierten Mekel-Zell-Karzinoma” - 90 year old female with locally advanced merkel cell carcinoma
- Chemotherapy can be used when patients fail to responde, are intolerant or contraindicated. Include in clinical trial
- Palliative RT may be considered when surgery is not feasible
Follow up guidelines
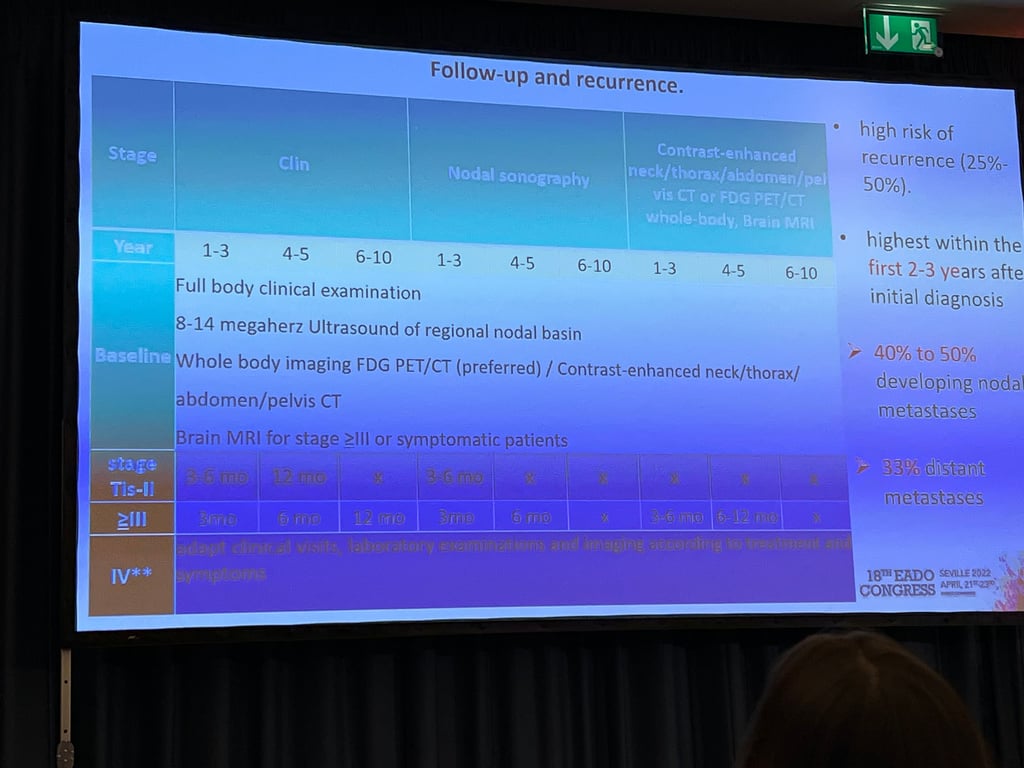
- High risk of recurrence (25-50%)
- Higher risk in first 3 years
- Even more aggressive than melanoma, so aggressive follow up
 Made with Bullet
Made with Bullet